Learn about Lipoedema, Our Multidisciplinary Approach & Treatment Options
Lipoedema
Lipoedema affects 1 in 11 women with abnormal fat deposition.
We offer
- Comprehensive consultation
- Diagnostic imaging / ICG where there is potential underlying lymphoedema
- Body contouring surgery and liposuction surgery
Lipoedema (also known as Lipedema) is a chronic disease or syndrome that was first reported by Allen and Hines in 1940.
Lipoedema mainly affects women, and is characterised by
- large/fat legs due to the abnormal subcutaneous fat deposition in the buttocks and lower limbs in variable distribution.
- The increase in volume in the lower extremities is often disproportionate to the rest of the body, sparing the feet.
- It can also affect the upper extremities, but sparing the hands.
- In severe cases, there is lymphoedema (the accumulation of fluid) in the legs due to impairment of the lymphatic vessels.
It is often painful with increased pressure sensitivity and easy bruising, and often starts between puberty and age 30s. It may occur with or without obesity.
The accumulated fat in lipoedema is resistant to dietary changes or caloric restriction, exercises or weight loss surgery. Hence, patients often feel helpless against the weight gain and may experience significant disability, finding it hard to perform activities of daily living, which can then lead to psychosocial distress. Severe lipoedema may cause joint damage.
As there are many systemic or local causes of leg swelling, it is often under-diagnosed or mis-diagnosed, and hence the prevalence is uncertain. The cause of lipoedema is also unknown but there may be a genetic or hereditary component, with the mother or grandmother experiencing similar disease.
According to the pattern of fat distribution, Schneider and Meier-Vollrath (2007) came up with a classification that distinguishes five types of lipoedema
Type I: Pelvis, buttocks and hips (saddle bag phenomenon);
Type II: Buttocks to knees, with formation of folds of fat around the inner side of the knee;
Type III: Buttocks to ankles;
Type IV: Arms;
Type V: Lower leg.
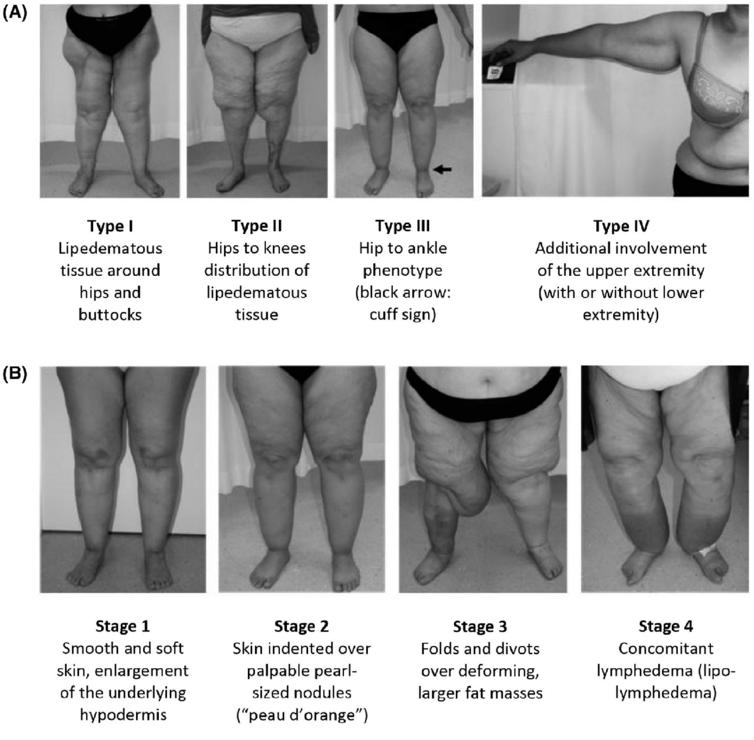
Figure 1 (A) Types and (B) stages of lipedema
Figure from Buso et al Obesity 2019
Treatment
Patients are best managed under multidisciplinary team, consisting of dietitian, exercise therapist, psychologist, lymphoedema therapist, physician and surgeon. As many patients have concurrent obesity, weight management through lifestyle modification is very important. Current treatment aims to reduce or improve the symptoms and to prevent disease progression. There are non-surgical and surgical treatments available. The former helps to decongest the fat tissue by helping to drain the ‘trapped’ fluid, whereas surgery such as liposuction is performed to reduce the fat tissue.
Non-surgical treatment includes:
- compression garment therapy or wrapping to reduce edema
- manual lymphatic drainage (MLD)
- complex decongestive physiotherapy (CDP).
- Consists of MLD, compression garment or bandage, decongestive exercises, and meticulous skin care.
- Can be combined with intermittent pneumatic compression (IPC).
However, many patients only achieve temporary success with the conservative therapy only. If there is no or minimal improvement after 6-12 months, surgical treatment is often indicated.
The mainstay of surgical treatment is tumescent liposuction, usually in several sessions due to high risk of morbidity associated with large volume liposuction of more than 4-6 litres in each session. We usually recommend an interval of 3 months between sessions. Patients should continue with the conservative therapy during these periods and also to ensure there is no significant weight gain as the fat can re-accumulate.
The technique of liposuction differs from the conventional liposuction techniques, with the care to avoid damage to the fragile lymphatic vessels. Hence, it requires more incisions than the conventional techniques.
It has been shown that tumescent liposuction is effective, not just for symptom relief, but also stopping disease progression and therefore, improve quality of life. It also reduces the amount of non-surgical treatment sessions.
Once adequate fat reduction is achieved, there is often excess saggy skin that may require surgical excision. The final procedure may involve lipectomy which means skin and fat are excised.
Reference

After 5 sessions of liposuction (Wiedner)
- Wiedner et al. Plast Aesthet Res 7:10, 2020
- Warren et al. Plast. Reconstr. Surg. 119, 2007.
- Buso et al. Obesity 27, 2019
- Bauer et al. Plast. Reconstr. Surg. 144, 2019